
Oxygen Uptake: Exercise and Voluntary respiration
Scientific literature on human physiology fails to empirically explore volitional breathing at frequencies below 8 br/min. At least, we todate have not been to find any study. Our organization has made a limited pilot study on three persons, all male, breathing at frequencies of 15, 8, 6, 5, 4 and 3 br/mi.
Person-1 is 80, Person-2 is 71 year old retired medical doctor and Peerson-3 is 55. They all are in excellent health. Person-1 put the study together and was responsible for gathering and interpreting thr data. Everybody was not tested at all breath frequencies. Perosn-1 was tested at all frequencies while the others ware tested at frequencies of 15, 8 and 4.
Our orgaization has no laboratory. Thus controls exercised on conducting the measurements were rather laboartory standard. It conducted this empirical study because of its interest in voluntary breathing and potential benefits in health, wellness and spiritual domains.
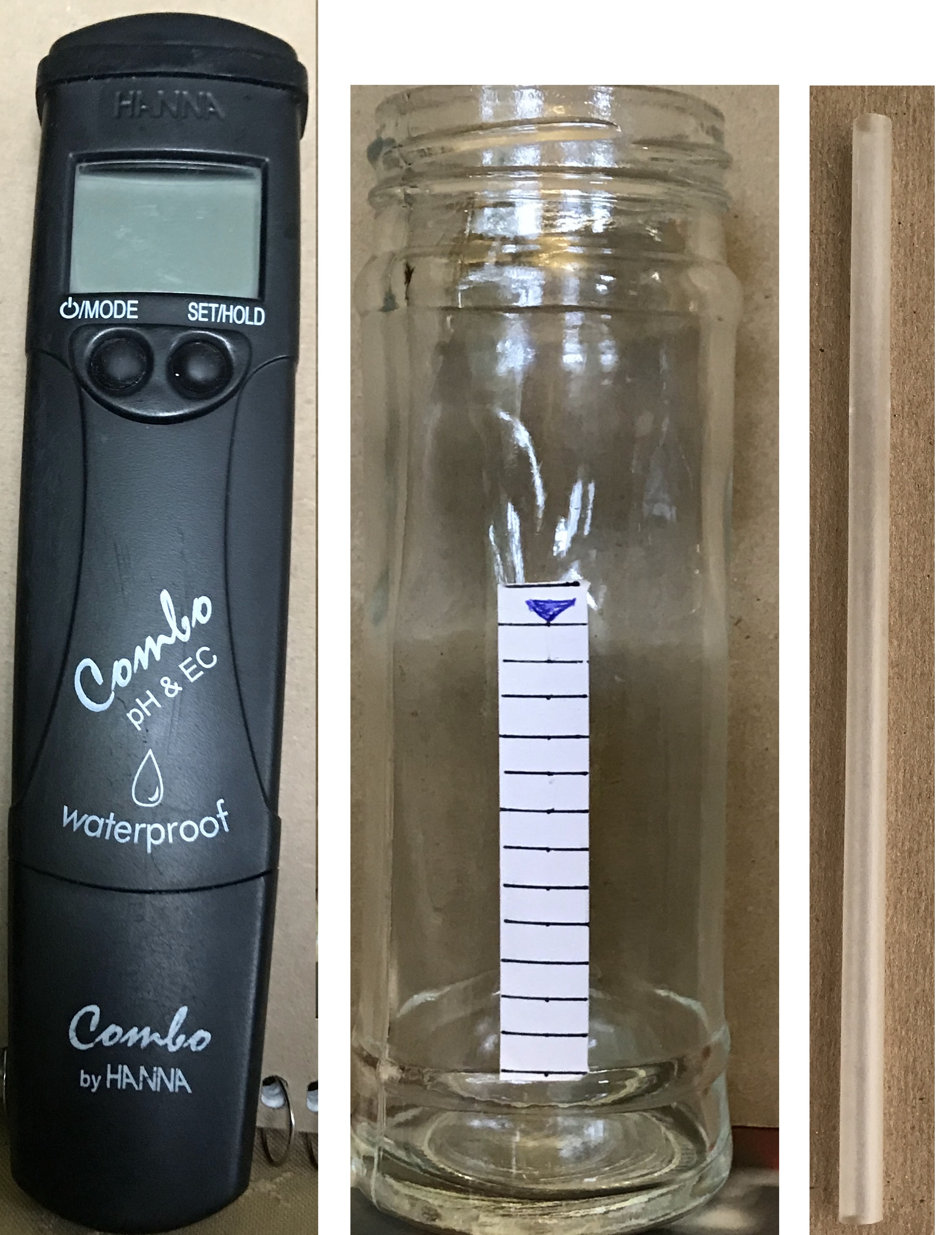
The test subject breathed in through his nose and out with the mouth through a straw with the other end at the bottom of a column of water in a glass jar. Between the readings of a person, the jar, the height of the column of water, water source, temperature of water etc. were kept the same as much as possible without laboratory faciilties. Standard time period of 5 minutes was used for every breath frequency. Carbon dioxide in the exhalation dissolving in the column of water changed the acaidity of water to different extents. We used a Combo pH meter to measure the acidity levels. The pH meter used was borrowed from a local envireonmental company. We hereby express our debt of gratitude to this company.
The figure below shows the apparatus used in our empirical observations. The height of the water column was upto the downward arrow mark on the jar. All water used in the study was from the kitchen tap. Best efforts were made to keep the tap setting the same during a set of measurements.
Inverse log to the base 10 of the difference between the pH value of the water column after breath frequency of 15 and another frequency is then the ratio of carbon dioxide exhaled at the other frequency to that at 15. this ratio also is the ratio between oxygen uptake at this other frequency and that at 15.
The following table summarises our results:
Table-1 Measured Oxygen Uptake with voluntary breathing by three men
|
Breath Frequency n |
Ratio of oxygen uptake at breath frequency of n br/min and |
||||
|
|||||
|
n = 15 br/min |
|
||||
|
n = 8 br/min |
|
||||
|
n = 6 br/min |
|
||||
|
n = 5 br/min |
|
||||
|
n = 4 br/min |
|
||||
|
n = 3 br/min |
|
The method we use is great for relative measurements of oxygen uptake. We must however take care to use an accurate and dependable pH meter because pH is a measure on logarithmic scale which magnifies any errors in measurement. Numbers in Table-1, because of their relative nature, may be regarded as accurate in their magnitude of value is concerned without strict laboaratory controls.
Numbers in Table-1 show a compelling increase in oxygen uptake with volitional breathing. It seems that there are these factors involved in this increase: (1) An icreased volume of inspiration and decrase effect of dead space at low rates of breathing, (2) Increased volume of inspiration because of focused effort in volitional breathing as compared to autonomic breathing controlled by our emotional states, (3) Focus emphasizing the use of diaphragm and abdomenal muscles over other respiratory muscles in volitional breathing while autonomic breathing seems more intercostal, and (4) The alveolar air has more of an opportunity of exchanging gases due to decreased breath frequency.
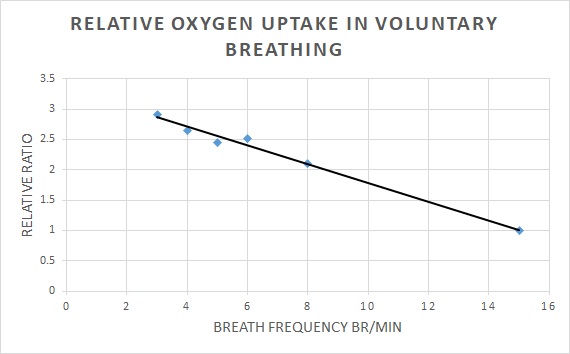
The following Figureis a graphical represention of the resultis in Table-1. Along the horizontal x-axis are breath frequency per minute and along the vertical y-axis are plotted the measured values of the ratio of oxygen uptake at a given breath frequency to that at the frequency of 15 br/min. Why 15 br/min? Because that is thought to be the avaerage value of autonomic frequency of human breath. The maximun value reachable by the trendline is 3.325. More research is needed to establish this number and the slope of the trendline.
We tried to interpret these realtive measurements in conjectured absolute terms. We can only do that making some basic assumptions. The absolute numbers can only be as good as these assumtions.
It is perhaps reasonable to assume that oxygen uptake is proportional to the alveolar volume. The alveolar volume at the autonomous frequency of 15 br/min, assuming tidal volume per breath of .4 litres and a dead space of 0.15 litres comes to 3.75 litres/min (see table at this link). We are going to use this value of alveolar volume of 3.75 at the frequency of 15 to work out the tidal and alveoar volummes at the frequencies of 3, 4, 5, 6 and 8 breaths per minute. The values calculated on this basis are given in the Table-2 below:
Table-2 comparing tidal and alveolar ventilation in exercise and voluntary breathing at different frequencies
|
Frequency of Braething br/min |
Air intake L/br |
Air intake L/min Vt |
Dead air L/br |
Va L/br |
Va L/min |
|
|
REST |
3 (volitional) |
3.84 |
11.52 |
0.15 |
3.69 |
11.07 |
|
4(volitional) |
2.54 |
10.16 |
0.15 |
2.49 |
9.94 |
|
|
5(volitional) |
1.99 |
9.95 |
0.15 |
1.84 |
9.19 |
|
|
6(volitional) |
1.72 |
10.32 |
0/15 |
1.57 |
9.41 |
|
|
8(volitional) |
1.14 |
9.12 |
0.15 |
.99 |
7.91 |
|
|
20 (autonomic) |
1 |
20 |
0.15 |
0.85 |
17 |
|
|
30 (autonomic) |
1.5 |
45 |
0.15 |
1.35 |
40.5 |
Note the alveolar volume number with autonomic breathing at the frequency of 8 is 4.8 litres/min (see table at this link). Comparing this value with that in Table-2 of 7.91 litres/min makes you think that this value is not dependent on the reate of breathing only. Other factors of voluntary breathing over and above the frequency of breathing influence the alveolar and tidal volumes.
The numbers in Table-2 for voluntary breath frequency of upto 8 br/min are compared with the numbers for automomic breathing during exercise. The numbers for alveolar volumes indiacte that volitional breathing is comparable to mild exercise. The numbers for oxygen uptake in Table-1 equally point in the same upward direction.
This comparison indicates that exercise is not the only approach to increase oxygen uptake. Volitional breathing provides an alternative. Unlike exercise,it does not require any work to be done by locomotive muscles. Practically, the entire increase in oxygen uptake with volitional deep breathing is available for nourishing the whole body. You can even say that physically volitional breathing is deeper rest simultaneously providing the benefits of mild exercise than rest while breathing autonomically.
Additionally, volitional breathing at low frequencies attenuate sympathetic dominance because of its association with parasympathetic actvity of the autonomic nervous system. Because of this reason, a regular practice of it can benefit all tissue structures and physiological functions innervated by the autonomic nervous system. Reduced sympathetic and increased parasympathetic actvity can also allevaite a whole horde of mental health and social behavior issues.
With regular practice of deep breathing, the practitioner can repalce the ordinary sympathetic domination with the dominance of parasympathetic activity. When that happens, the effort applied in breathing at low frequencies reduces, mental focus sets in drastically reducing mental activity, and breath frequencies can approach almost zero. With almost negligible breath activity, body is kept alive with the abundane of energy stored from the excess produced in the process of deep breathing that gets the practitioner there.
Table 3 - Air Intake/br and Alveolar Air L/min with breath frequency from 0 to 40 br/min
|
Br/min |
Air intake L/br |
Alveolar Volume L/min |
Remark |
|
0 |
0 |
0 |
|
|
1 |
3.84 |
3.69 |
extrapolition |
|
2 |
4 |
7.7 |
extrapolition |
|
3 |
3.84 |
11.07 |
volitional |
|
4 |
2.54 |
9.94 |
volitional |
|
5 |
1.99 |
9.19 |
volitional |
|
6 |
1.72 |
9.41 |
volitional |
|
8 |
1.14 |
7.91 |
volitional |
|
15 |
0.4 |
3.75 |
|
|
20 |
0.3 |
3 |
|
|
40 |
0.15 |
0 |
Figure below is a graphical representation of the numbers in Table 3 for air intake per breath. Note the dotted line representing the air intake per breath with autonomic breathing. Especially noteworthy is the difference in the air intake for the breath frequency of 8 br/min with volitional breathing (solid curve) and its value for the same breath frequency with autonomic breathing (dotted line). It seems that this volume depends not only on breath frequency but also on whether the breathing is volitional or autonomic.
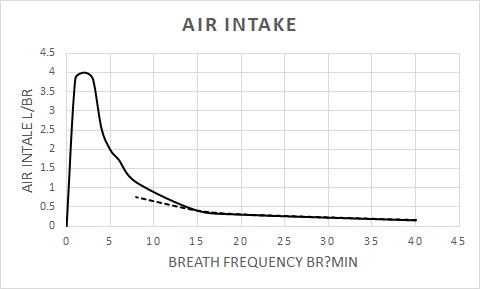
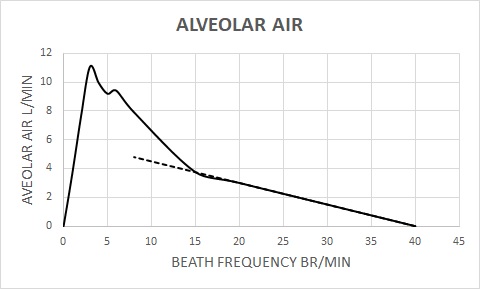
Figure below is a graphical representation of the numbers in Table 3 for alveolar air in L/min. Note the dotted line representing the alveolar air L/min with autonomic breathing. Again, note the difference in the alveolar volume for the breath frequency of 8 br/min with volitional breathing (solid curve) and its value for the same breath frequency with autonomic breathing (dotted line). It seems breath frequency together with the process of breathing, whether volitional or autonomic, makes a difference to alveolar volumes.
This pilot study conclusively shows the effectiveness of deep breathing in improving oxygen uptake by its practitioner. The practical usefulness of higher oxygen consumption in the potential health benefit that can accrue to the public at large, and in particular to the handicapped, the seniors, sick, shut-ins or those in the hospital being treated or recovering from surgery. In addition, deep breathing results in many other potential health and wellness benefits from a reduction in sympathetic dominance and neural restructuring.
In addition, it points to a gaping hole in the understanding of the power of the breath at frequencies outside the range of natural homeostasis. There is a whole range of physiology that needs professional and scientific exploration with the promise of a whole range of potential benefits in multiple areas of physical health, mental health, wellness, social behavior, and learning ability. Because of the inter-connection of breath and the nervous system, this research can lead to a re-examnination of the basic model of mind-body interconnectivity in health care with possibilities of fundamental and revolutionary changes.
Cancer may not be curable but it certainly seems prevetable with increased oygen uptake through voluntary respiration. This report of incresed oxygen uptake with volitional breathing may perhaps be read in the light of Dr. Wlburg's cancer hypothesis according to which cancer growth is caused by tumor cells generating energy (adenosine triphosphate/ATP) mainly by anaerobic cellular respiration in contrast to healthy cells which mainly generate energy from aerobic respiration (https://en.wikipedia.org/wiki/Otto_Heinrich_Warburg).
Cancer, above all other diseases, has countless secondary causes. But, even for cancer, there is only one prime cause. Summarized in a few words, the prime cause of cancer is the replacement of the respiration of oxygen in normal body cells by a fermentation of sugar.
— Otto H. Warburg,
Finally, we invite researchers in human physiology to independently verify the results reported herein. We also request interested researchers to comment and make suggestions on this report via e-mail to info@spiritualeducation.org.